
New Study Verifies How Cholesterol Lowering Statin Drugs Injure Muscles - A Drug 40 Million Americans Take

We are seeing the gradual dismantling of the Big Pharma propaganda regarding vaccine safety, childhood vaccine schedule and the incentive payments for physicians. That is huge progress in reversing the unscientific politicization and influencing patient physician relationships through money - called pay for performance.
Doctors Will No Longer Receive Financial Rewards for Vaccinating Kids
Another big area factoring into physician pay for performance bonuses is the prescription of cholesterol lowering statin drugs. About 40 Million Americans currently take statins. Many bonus incentive programs of health care providers are based on Center of Medicare pay for performance metrics that were implemented two decades ago and now have evolved to affect every area of medical care given.
MEDICARE “PAY FOR PERFORMANCE (P4P)” INITIATIVES
The integration of medical records systems have provided for continuity of care purposes transferable and accessible records within large health care systems about these metrics tied to physician reimbursement. These are “standards of care”, and anybodies cholesterol that is above a set very low goal number is automatically alerted to the provider for the initiation of statin drug prescription. This is reinforced by Insurance companies who send letters to clinicians who are not meeting “standards of care”.
The idea that high cholesterol causes atherosclerosis has been fundamentally debunked by great cardiologist Dr. Thomas Levy decades ago. His books explaining that Vitamin C deficiency is the primary driver of atherosclerosis have provided important paradigm shifting information and insights, ignored by the Big Pharma aligned health care system. Additionally, it is known that toxic heavy metals cause artherosclerosis as well. While published in reputable medical journals, these causes are ignored by conventional medical doctors and cardiologists:
Low-Level Environmental Exposure to Lead Unmasked as Silent Killer
Menke et al7 analyzed the database of the Third National Health and Nutrition Examination Survey (NHANES III) to investigate the relation between total and cause-specific mortality and blood lead in a representative sample of the US population. All 13 946 participants (≥17 years of age) included in the analysis had a blood lead concentration <0.48 μmol/L (10 μg/dL). (To convert micromoles per liter of lead into micrograms per deciliter, multiply by 20.712.) Follow-up lasted until December 31, 2000. With adjustments applied for confounders, subjects in the highest third of the blood lead distribution (≥0.17 μmol/L), as compared with those in the lowest third (<0.09 μmol/L), experienced a significantly higher risk of death. Estimates of the excess risk amounted to 25% and 55% for total and cardiovascular mortality, respectively, and 89% and 151% for myocardial infarction and stroke.
Just like I have in my office for years reversed Atherosclerosis verifiably with EDTA Chelation, Vitamin C and Nitric Oxide supplementation, Dr Levy also has advocated for these methods and explained their medical validity from the viewpoint of orthomolecular medicine. Since statins are known mitochondrial toxins, he also advocated for decades against them.
You can see our important interview here:
Dr Levy also alerted me that Antimony and other toxic metals directly are correlated with congestive heart failure in published studies, and since these metals are ubiquitous in vaccinations and sprayed on us via geoengineering operations, hence also affecting our food and water supply - this is another ignored correlation of direct environmental risk contributing to cardiac disease.
One of my all time favorite medical books is Stop America’s #1 Killer - Proof that the origin of all Coronary Heart Disease is clearly reversible Arterial Scurvy ( Vitamin C deficiency). I highly recommend it to my readers.
One of the first tests I do when patients come to my office is a Urine Vitamin C level. Over 80% of people who have not already been listening to my interviews on Vitamin C have scurvy. I follow Linus Paulings recommendation of up to 10000mg ( ten thousand) Vitamin C daily according to bowel tolerance, great for reversing a lot of chronic diseases. These are some of Dr Levy’s books.
Dr Levy’s findings were supported by another great cardiologist, who bravely published papers regarding the evidence that statins in fact increase atherosclerosis and congestive heart failure, hence making people worse. This is the article showing that statins increase congestive heart failure and atherosclerosis.
Statins stimulate atherosclerosis and heart failure: pharmacological mechanisms
In contrast to the current belief that cholesterol reduction with statins decreases atherosclerosis, we present a perspective that statins may be causative in coronary artery calcification and can function as mitochondrial toxins that impair muscle function in the heart and blood vessels through the depletion of coenzyme Q10 and 'heme A', and thereby ATP generation. Statins inhibit the synthesis of vitamin K2, the cofactor for matrix Gla-protein activation, which in turn protects arteries from calcification. Statins inhibit the biosynthesis of selenium containing proteins, one of which is glutathione peroxidase serving to suppress peroxidative stress. An impairment of selenoprotein biosynthesis may be a factor in congestive heart failure, reminiscent of the dilated cardiomyopathies seen with selenium deficiency. Thus, the epidemic of heart failure and atherosclerosis that plagues the modern world may paradoxically be aggravated by the pervasive use of statin drugs. We propose that current statin treatment guidelines be critically reevaluated.
Of course doctors like us who have gone against the mainstream narrative have been persecuted and marginalized. I remember a cardiologist telling one of my patients that I should loose my license for not prescribing statins. Interestingly, I reversed that patients atherosclerosis, subsequent ischemia and congestive heart failure with my methods, leaving these colleagues uncomfortably silent. Often the discharge summaries will say, patient opts for chelation therapy instead of triple bypass.
Recent studies have confirmed reversal of heavy atherosclerosis with EDTA - nanoparticles are unnecessary, regular EDTA has been used for this purpose for a century:
Conclusions: This is the first study showing the removal of calcium from heavily calcified arteries by using intravenous targeted EDTA therapy. Such therapy also reversed vascular smooth muscle cell osteoblastic transition and apoptosis in the arterial tissue, thereby potentially creating an environment for suitable tissue repair.
Similar articles
Arora S, Halsey G, Zohora FT, Swiss A, Vyavahare N.Int J Immunopathol Pharmacol. 2025 Jan-Dec;39:3946320251391142. doi: 10.1177/03946320251391142. Epub 2025 Dec 15.PMID: 41399092Free PMC article.
Karamched SR, Nosoudi N, Moreland HE, Chowdhury A, Vyavahare NR.Sci Rep. 2019 Feb 22;9(1):2629. doi: 10.1038/s41598-019-39639-8.PMID: 30796300Free PMC article.
Lei Y, Nosoudi N, Vyavahare N.J Control Release. 2014 Dec 28;196:79-86. doi: 10.1016/j.jconrel.2014.09.029. Epub 2014 Oct 5.PMID: 25285609Free PMC article.
Fulgenzi A, De Giuseppe R, Bamonti F, Vietti D, Ferrero ME. Efficacy of chelation therapy to remove aluminium intoxication. J Inorg Biochem. 2015 Nov;152:214-8. doi: 10.1016/j.jinorgbio.2015.09.007. Epub 2015 Sep 24. PMID: 26404567.
Of course historical humans studies have shown beneficial effects for years, but there are many people spreading disinformation and the FDA historically has waged war against EDTA:
Efrain Olszewer MD, James Carter MD EDTA Chelation Therapy: A Retrospective Study of 2870 Patients. J Adv Med 1989;2:197-211
Retrospective study EDTA chelation in 470 patients with peripheral vascular disease. Improvement 80-91%. Of 92 patients referred for surgical intervention only 10 required ultimate surgery saving an estimated 3 Million Dollars of insurance money. No adverse effects over 6 years.
Here are more systemic studies showing remarkable improvements:
Maybe the new evidence coming forward will change clinicians mind regarding their practices. However, that will never happen if the financial incentives do not change.
This new article now shows how statins injure muscles. Our heart is a muscle and is not excluded from this injury. The authors from Columbia University call for a reevaluation of statin therapy. I think this issue should be high on the MAHA agenda, since 40 Million Americans are having their mitochondria, the powerhouse of the cells, injured by statin drugs. Mitochondrial dysfunction can contribute to all diseases of aging.
Even Web MD talks about the substantial side effects -
The most common statin side effects include:
Headache
A hard time sleeping
Flushing of the skin
Muscle aches (myalgia), tenderness, or weakness
Drowsiness
Dizziness
Nausea or vomiting
Belly cramping or pain
Bloating or gas
Diarrhea
Constipation
Rash
Low levels of blood platelets
Less common side effects you may have with statins are:
Nausea
Hair loss
Pins and needles sensations, such as pricking, numbness, or tingling on your skin
Liver inflammation, which can make you feel like you have the flu
Pancreas inflammation, which can cause stomach pain
Skin problems such as rashes or acne
Sexual problems, such as erectile dysfunction or a low sex drive
Statins also carry warnings that memory loss, mental confusion, neuropathy, high blood sugar, and type 2 diabetes are possible side effects. It’s important to remember that statins may also interact with other medications you take.
Adequate Vitamin C levels can help lower cholesterol, studies referenced can be found in Dr. Levy’s book. I use Citrus Bergamot, a polyphenol, in my patients with statin intolerance
Clinical application of bergamot (Citrus bergamia) for reducing high cholesterol and cardiovascular disease markers
Here is the article:
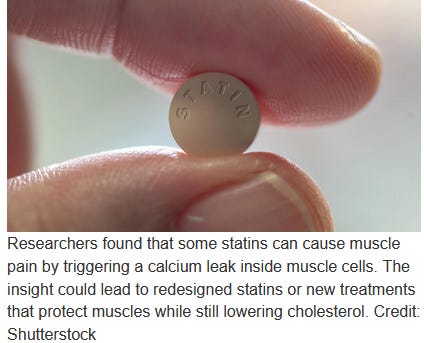
Scientists finally uncover why statins cause muscle pain
Summary:
A new discovery may explain why so many people abandon cholesterol-lowering statins because of muscle pain and weakness. Researchers found that certain statins can latch onto a key muscle protein and trigger a tiny but harmful calcium leak inside muscle cells. That leak may weaken muscles directly or activate processes that slowly break them down, offering a long-sought explanation for statin-related aches.
__________________________________________________________________________
Many people who are prescribed statins to lower cholesterol end up stopping the medication because of muscle pain, weakness, or ongoing fatigue. These symptoms are among the most common reasons patients abandon the drugs.
New research from Columbia University suggests a possible explanation for why this happens in some individuals. The study indicates that certain statins can attach to a protein inside muscle cells, triggering a leak of calcium ions that disrupts normal muscle function.
“It is unlikely that this explanation applies to everyone who experiences muscular side effects with statins, but even if it explains a small subset, that’s a lot of people we could help if we can resolve the issue,” says Andrew Marks, chair of the Department of Physiology and Cellular Biophysics at the Vagelos College of Physicians and Surgeons.
Statins are widely used in the United States. Roughly 40 million adults take them to control cholesterol levels, and about 10 percent develop muscle related side effects.
“I’ve had patients who’ve been prescribed statins, and they refused to take them because of the side effects. It’s the most common reason patients quit statins, and it’s a very real problem that needs a solution,” Marks says.
A Longstanding Puzzle Around Statin Muscle Pain
Scientists have been trying to understand statin related muscle problems since the drugs first became available in the late 1980s. Statins work by binding to an enzyme involved in cholesterol production, but they can also attach to other unintended targets in the body.
Earlier research hinted that muscle side effects might occur when statins interact with a specific protein in muscle tissue. Until now, the details of that interaction were unclear.
Using cryo-electron microscopy, a powerful imaging method that allows researchers to see structures down to individual atoms, the Columbia team was able to directly observe how a statin interacts with muscle cells.
Calcium Leaks Inside Muscle Cells
The images showed that a commonly prescribed statin, simvastatin, binds to two specific sites on a muscle protein known as the ryanodine receptor. This binding opens a channel in the protein, allowing calcium to leak into areas of the cell where it does not normally flow.
According to Marks, this calcium leak may explain muscle pain and weakness linked to statins. The excess calcium can weaken muscle fibers directly or activate enzymes that gradually break down muscle tissue.
Toward Safer Cholesterol Drugs
The findings point to new possibilities for reducing statin side effects. One approach would be to redesign statins so they continue to lower cholesterol but no longer bind to the ryanodine receptor in muscle cells.
Marks is currently working with chemists to develop statins that avoid this unwanted interaction.
Another potential strategy focuses on stopping the calcium leak itself. The researchers showed that in mice, statin related calcium leaks can be closed using an experimental drug created in the Marks laboratory for other disorders involving abnormal calcium flow.
“These drugs are currently being tested in people with rare muscle diseases. If it shows efficacy in those patients, we can test it in statin-induced myopathies,” Marks says
Study Details and Disclosures
Andrew Marks is also the Clyde and Helen Wu Professor of Medicine at Columbia University Vagelos College of Physicians and Surgeons, a professor of biomedical engineering, and director of the Wu Center for Molecular Cardiology.
The study was published Dec. 15 in “Structural basis for simvastatin-induced skeletal muscle weakness associated with RyR1 T4709M mutation,” in the Journal of Clinical Investigation.
Gunnar Weninger, Haikel Dridi, Steven Reiken, Qi Yuan, Nan Zhao, Linda Groom, Jennifer Leigh, Yang Liu, Carl Tchagou, Jiayi Kang, Alexander Chang, Estefania Luna-Figueroa, Marco C. Miotto, Anetta Wronska, Robert T. Dirksen, Andrew R. Marks. Structural basis for simvastatin-induced skeletal muscle weakness associated with type 1 ryanodine receptor T4709M mutation. Journal of Clinical Investigation, 2025; 135 (24) DOI: 10.1172/JCI194490
Yes, metals in the body and brain are the root cause of Many 'diseases' and 'syndromes'.
Just do a websearch for 'Any Disease' and 'metals' (not all bad metals are 'heavy).
And EDTA and ascorbic acid does Many Many good things, aside from being The Best OTC oral chelator there is. Period.
And they have essentially cured or greatly improved many of those same medical conditions with EDTA.
Now do the same websearch for 'Any Disease' and 'EDTA'.
There are many many bullshit fearporn articles out there about it (because its Great) so you will need to go through several pages of results but if you look long enough, there is Always an EDTA study (or six) about That disease. Many from the 50's and 60' and 70's.
Because its been around since the 1930's, just as long as Ascorbic Acid/Vitamin C.
And there is Nothing Else like it, which is why they use it to bind to metals in so many studies.
There are hundreds of Thousands of studies going back 90 years about EDTA.
Millions of people have taken it for Decades and millions more just since Dr Ana started recommending it.
No Deaths, no issues, just like All of Dr Anas evidence up above. With Millions of people Globally.
And tbh, most people are taking very very low amounts anyway when you consider the old studies where people took 27 Grams of oral calcium disodium EDTA a Day for over a Year.
And if you have been eating charcoal and/or have been misled into thinking EDTA can do anything to graphene, dont worry, EDTA doesnt bind with carbon whatsoever. Period.
Its in Many studies, Read Them or listen to people that Have.
And if we are going to be honest, no one has proven via a basic carbon Chemical test that it Is in fact Graphene. Why Not? Thats a Simple test.
And RAMAN spectroscopy is Comparative, it Only shows that the stuff in the vaxxes and dental anesthetic gives off a Similar Spectrum of light To graphene.
If it were a novel or previously unknown element, RAMAN would not know what it is.
And as these jabs can do things beyond our understanding of conventional physics, it stands to reason that of course there are things we do not publicly know about in them.
Luckily EDTA is so great, not only will it bind with rare metals no one even looks for, like plutonium or neptunium, they think it most likely even binds with metals we have not even Discovered or produced in mass yet.
EDTA IS GREAT, which is why there are so many mainstream fearmonger articles about it out there. What, do you think they are trying to Help You all of a sudden?
And yet even with allllll the EDTA fearpprn, they still cannot find a single death or injury from oral EDTA.
Ever.
And its Nontoxic.
And available Over The Counter.
Haha, yeah, sounds pretty scary.
Ohhhh, be Very Scared...
of removing metals from your body!!!
Oh wait, you might remove Too Many Metals... be Very Scared of that Toooo!!
Lol, I've taken more than anyone else and I never ever supplement with minerals but feel free, if it makes you feel better.
I dont think anyone needs it though, unless they have a pre-existing mineral issue or imbalance.
Just make sure you take EDTA/C right though or it Wont Work.
https://arizonanatural.com/blogs/edta-resource-hub/3-common-mistakes-made-when-taking-edta
If you Do though, Its fuggin Great.
It does So many good things that I regularly waste my time to tell you about it.
Also dont take statins, but none of the blood thinners in the world will completely fix the self-replicating blood polymerization, no matter how much you take.
Theres a long list of them, including some 'natural' ones but you know what Will slowly stop and reverse it?
EDTA and ascorbic acid. Choose to live people.
More slow kill by big pharma . 🤬